Discover how today’s most successful IT leaders stand out from the rest. Read the report
Meet Asana Intelligence
AI has joined the team to help executives, departments, and entire organizations work smarter.

Drive clarity and accountability
Take the guesswork out of strategic planning and hit business-critical goals

Maximize impact
Boost everyone's productivity by using AI to create and improve workflows

Scale with confidence
Unify teams, tools, and work data with security and reliability
DRIVE CLARITY AND ACCOUNTABILITY
Set and hit business-critical goals with confidence
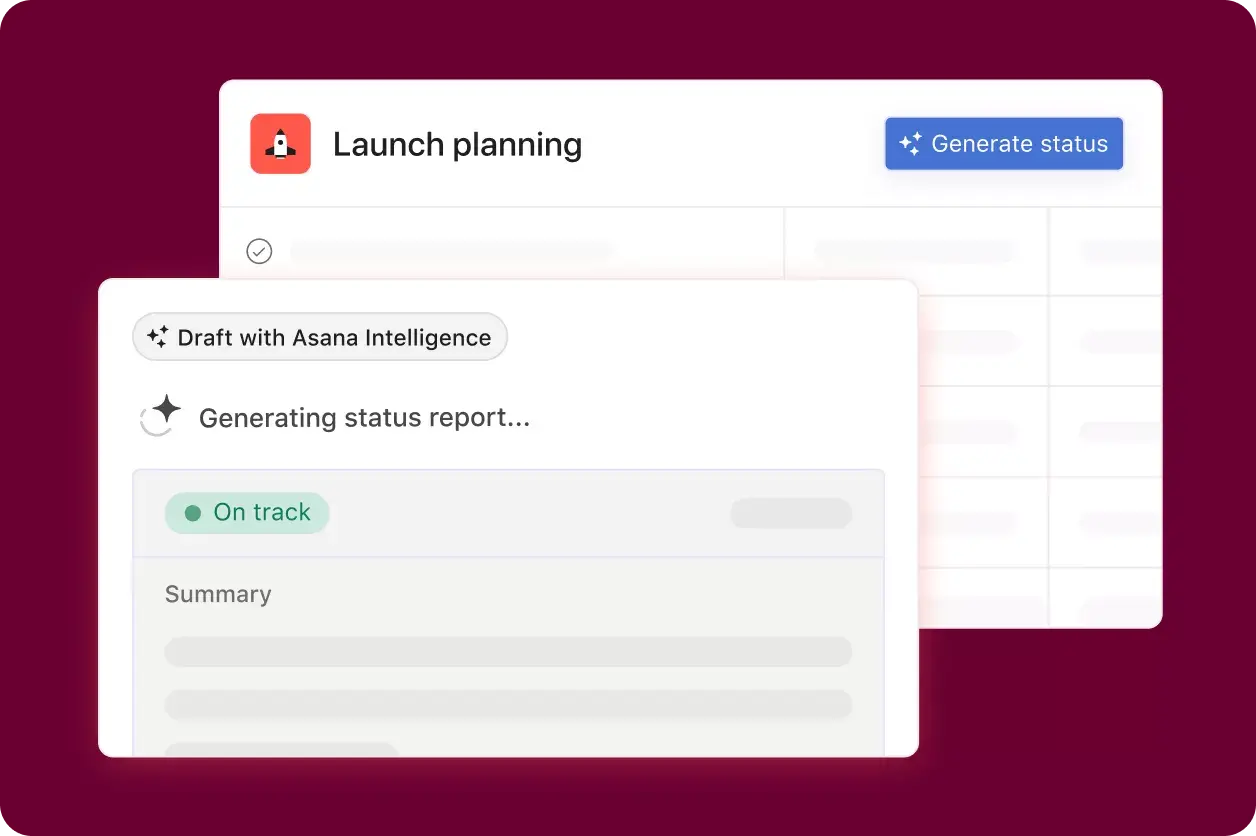
Smart status
Create status updates faster on goals, portfolios, and projects, with AI pulling from real-time work data to identify risks, roadblocks, and open questions.

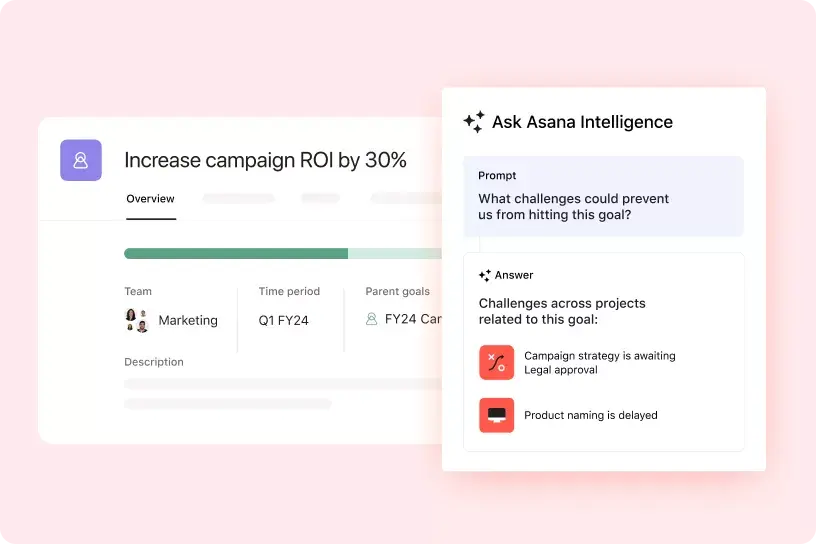
Smart answers
Ask Asana questions about your tasks and projects to get timely insights, identify challenges, and determine next steps.
Coming soon to goals and portfolios.
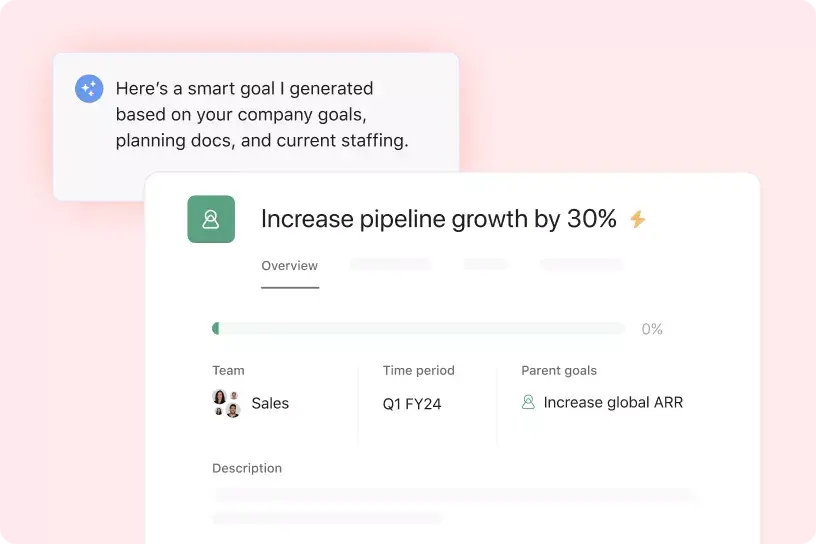
Smart goals
Write down more effective goals and standardize them across your organization. With the help of AI, get suggested tips to draft goals based on best practices.
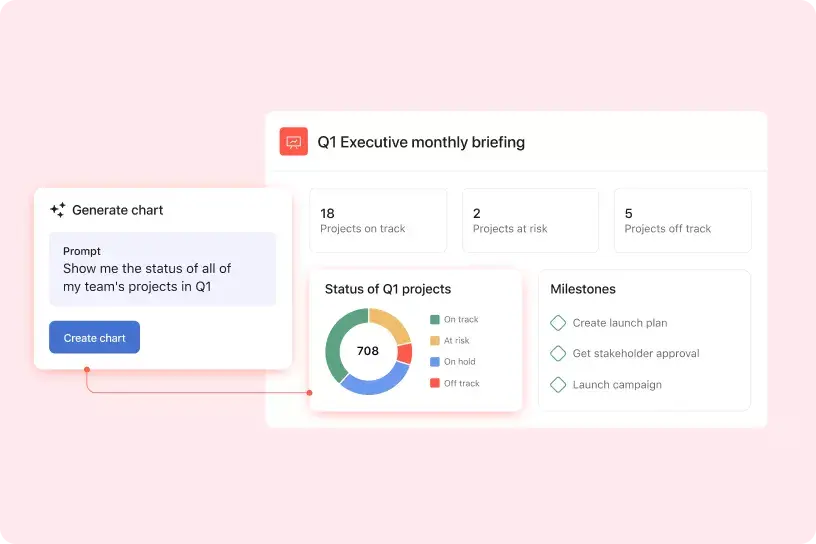
Smart reporting
Make it easy for everyone to see and understand how work is progressing. Tell AI what data you want to visualize and get help creating charts automatically.
IT professionals using Asana are 57% more likely to be confident their organization is prepared for AI¹
Discover the challenges and opportunities facing today's IT leaders-and what sets apart high-performing ones.
MAXIMIZE IMPACT
Build workflows faster and boost productivity

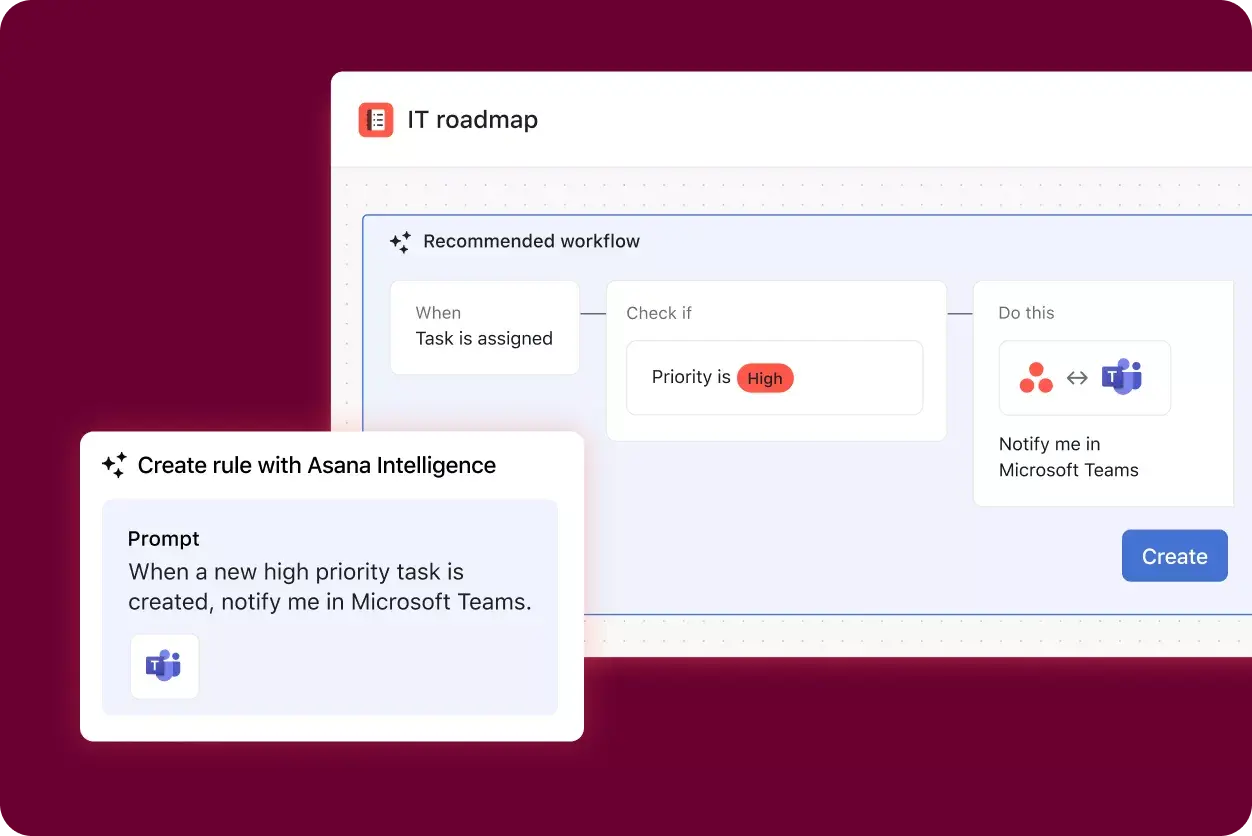
Smart workflows
Give AI a few simple instructions and it will build workflows optimized to match specific goals and best practices.

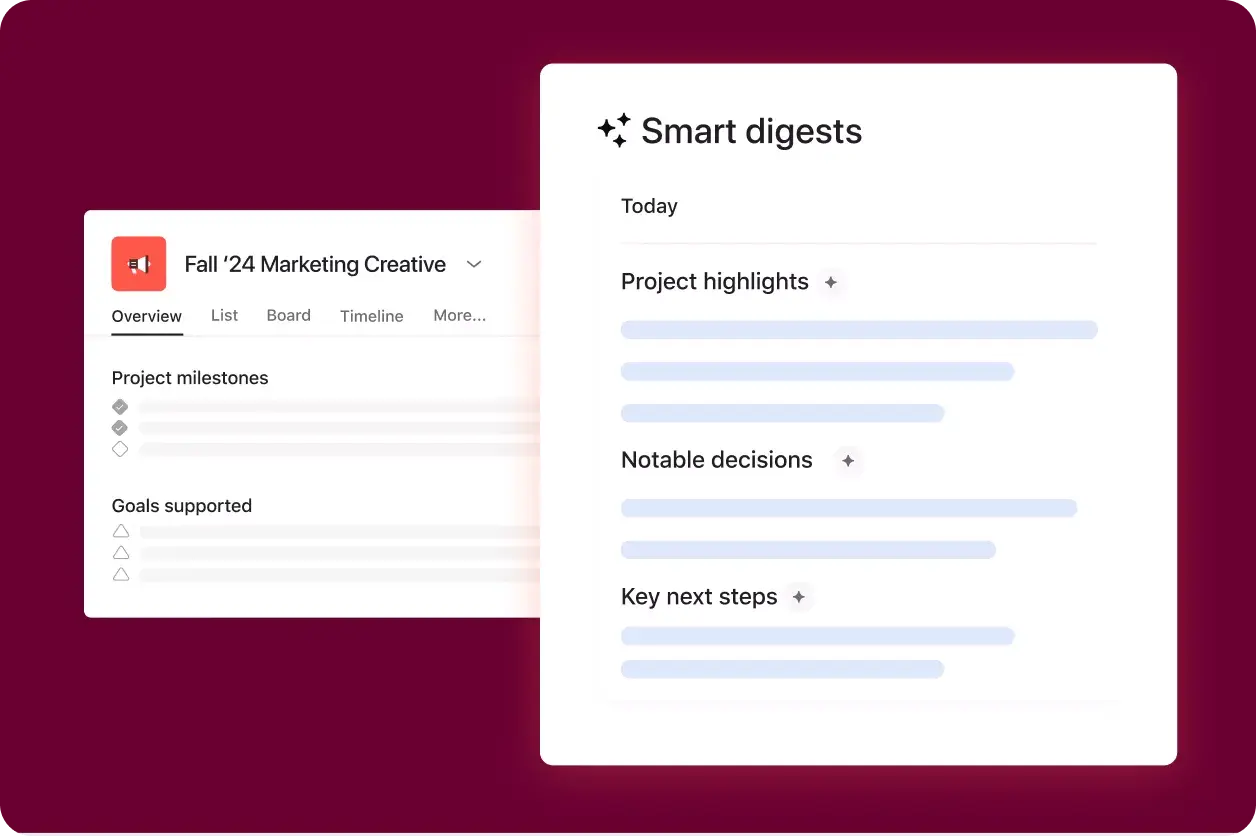
Smart digests
Get a short summary of what's happened in a project during a specific time frame, so you can get up to speed on any notable changes.
Smart summaries
Review action items and highlights from tasks and comments without another meeting. You can also summarize tasks instantly in Slack.
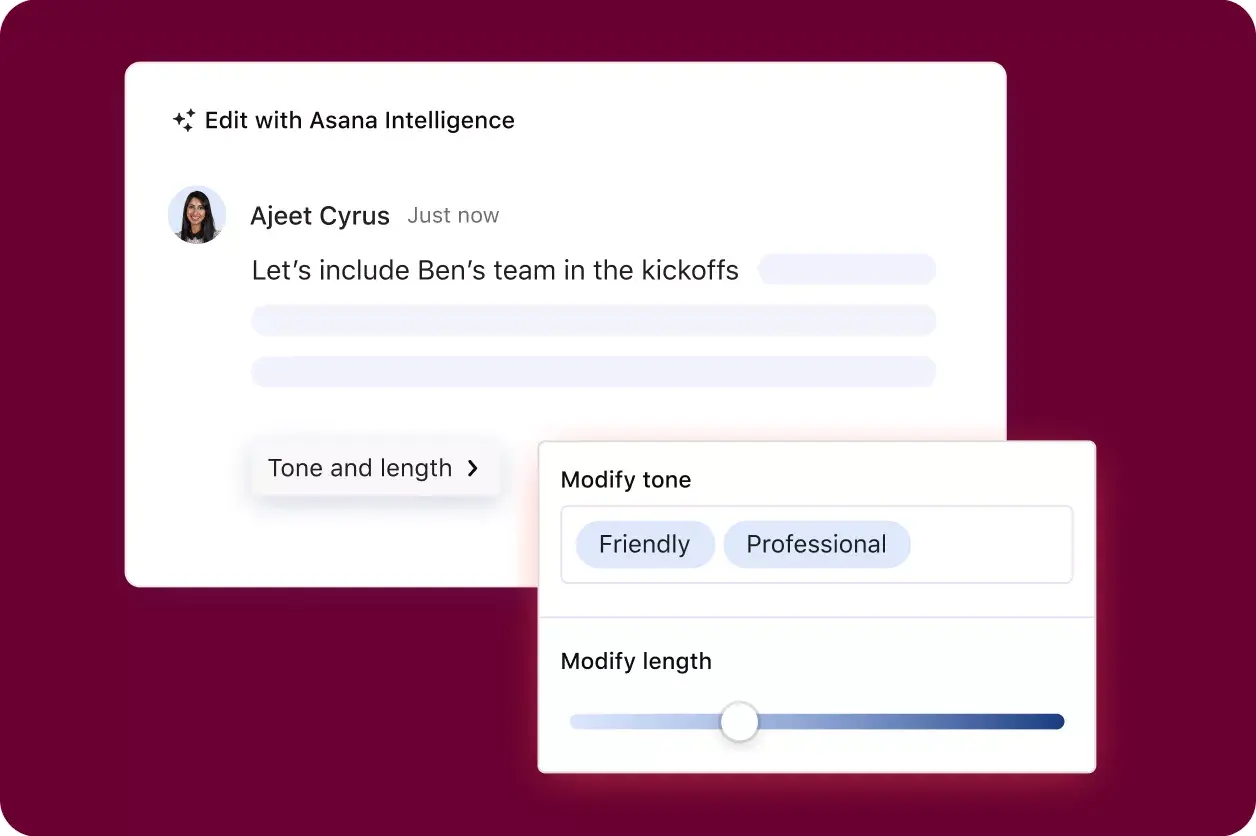
Smart editor
Write clearer, more compelling responses that strike the right tone and improve your formatting.
Asana is committed to AI safety and transparency

Our AI partners do not use your data to train their models.
Our AI partners are required to delete customer data after each query.
SCALE WITH CONFIDENCE
Scale work easily with trusted security and reliability
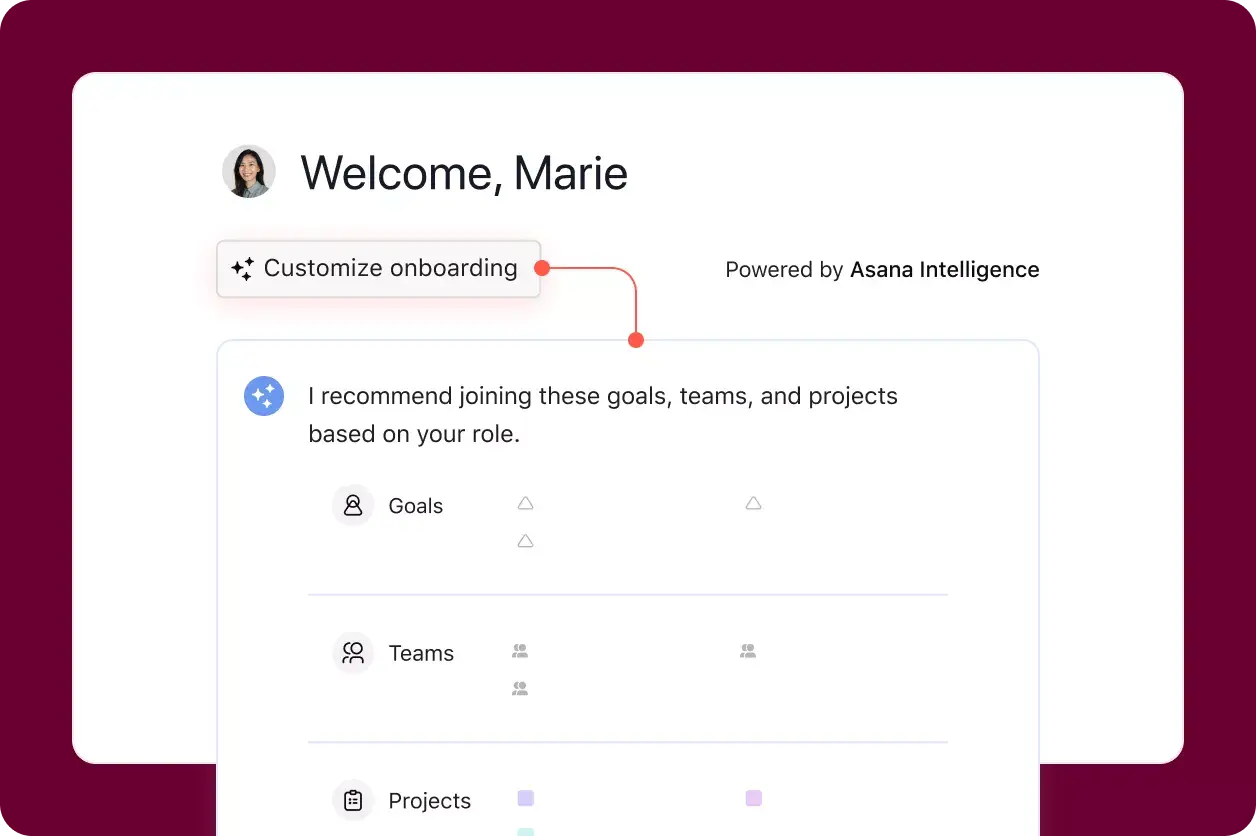
Smart onboarding
Help new hires get up to speed on the right projects, teams, and goals so they can drive immediate impact.
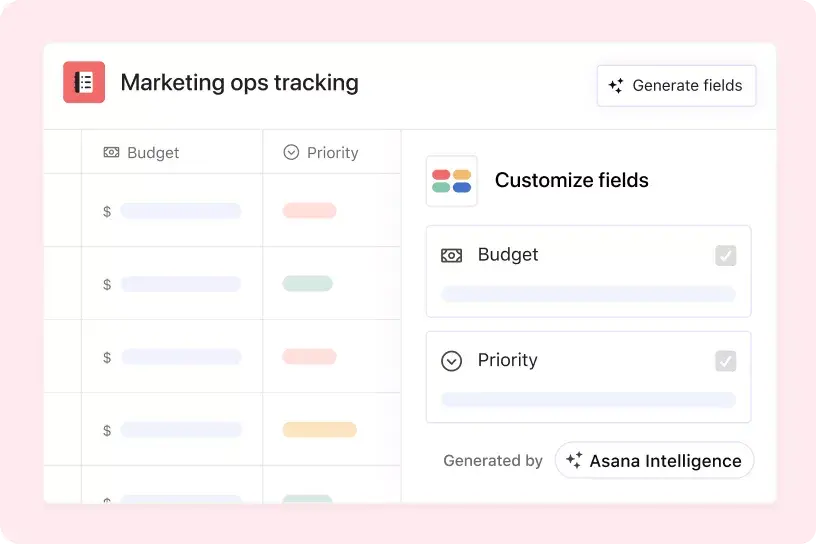
Smart fields
Organize projects to support collaboration with auto-generated custom fields.
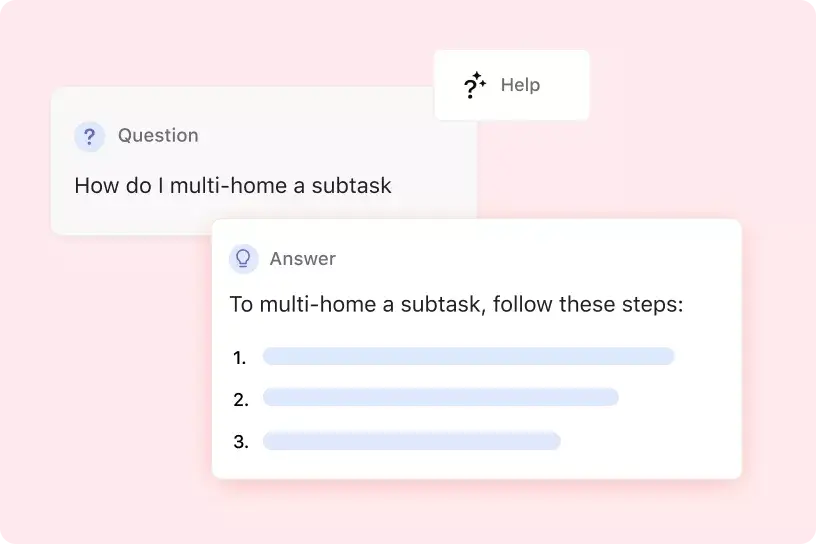
Smart help
Get in-product help and expert tips on using Asana.
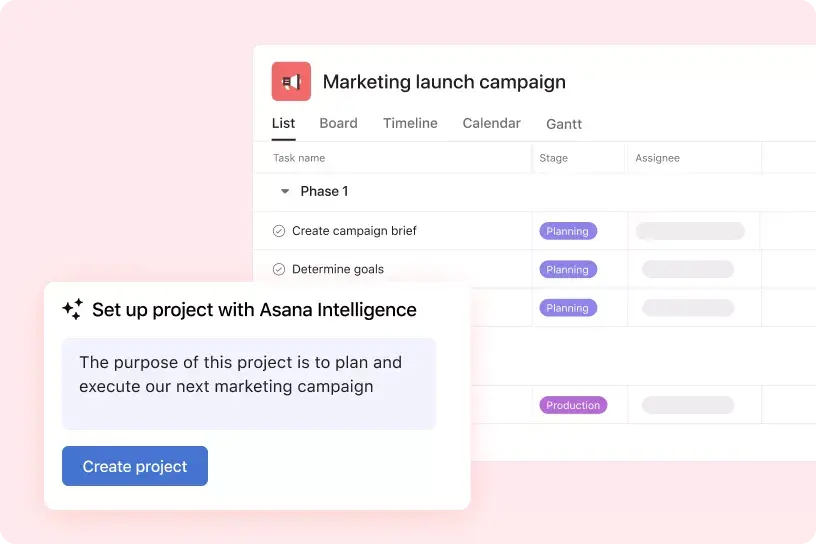
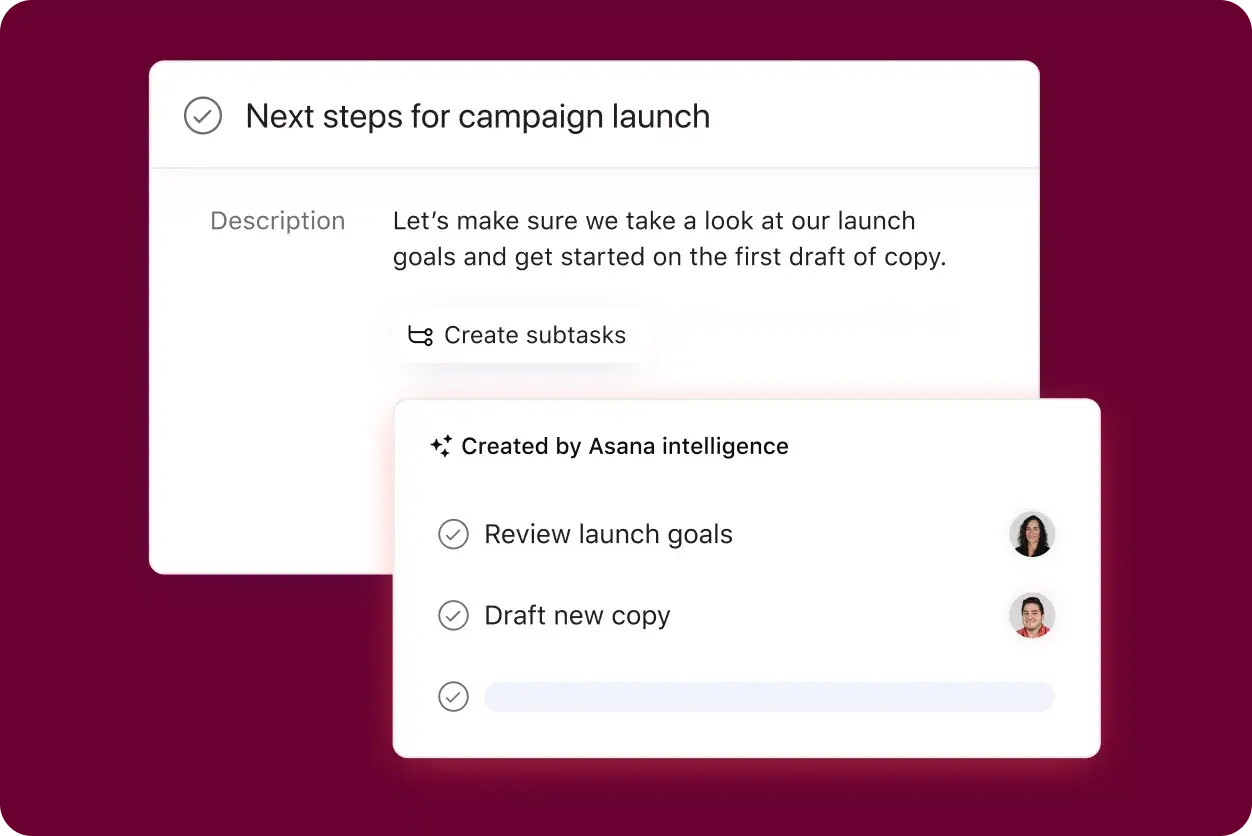
Smart projects
Tell AI about your next project and it will build one with the right structure for you.
Asana’s guiding principles for human-centered AI
Learn how we're empowering teams to work together more effectively and efficiently.
AI features powered by the most complete and connected map of your organization's work data - the Asana Work Graph®
Go deeper
Automating your workflows is just the start. See what else you can do with Asana.

Project and task management
Track work from start to finish so every team knows exactly what to do to hit their goals.

Goals and reporting
Connect daily work to company-wide objectives, and track progress in real time.

Workflow automation
Create processes that run themselves, so teams can focus on the next big thing.

Admin and security
Scale with confidence and keep your company’s work safe.
From workflows to workloads - we've got you
1. Compared to IT professionals not using Asana.